ASCO awards Eduardo Vilar-Sanchez, M.D., Ph.D., for cancer prevention research | ASCO 2026
Congratulations to CPI scientist Eduardo Vilar-Sanchez, MD, PhD, who has been recognized by the American Society of Clinical Oncology (ASCO) with one of the society’s highest honors as the 2026 recipient of the ASCO—American Cancer Society Cancer Prevention Award.
ASCO Congratulates 2026 Special Award Recipients | ASCO Connection
ASCO-American Cancer Society Cancer Prevention Award 2026
Eduardo Vilar-Sanchez, MD, PhD
Dr. Vilar-Sanchez is professor and Chair, ad interim, of the Department of Clinical Cancer Prevention, at the University of Texas MD Anderson Cancer Center. He is a physician-scientist and medical oncologist specializing in Hereditary Cancer syndromes, with a focus on Lynch Syndrome (LS) and Familial Adenomatous Polyposis (FAP). His work bridges the gap between molecular discovery and clinical application, aiming to understand colorectal carcinogenesis and develop novel cancer interception strategies. His lab is at the forefront of identifying neoantigens for preventive vaccines and exploring how pharmacological agents, like naproxen, and lifestyle interventions, such as exercise, modulate the immune environment. Through these efforts, Dr. Vilar-Sanchez is transforming cancer prevention into a personalized, proactive discipline for genetically predisposed patients and their families.
Lyda Hill Philanthropies backs CPI’s cancer prevention research with $750k challenge grant
DALLAS, TX — [December 3, 2025] — Underscoring the growing momentum behind the prevention-first approach to cancer, the Cancer Prevention Initiative (CPI) today announced a $1.5 million funding opportunity made possible by a commitment from Lyda Hill Philanthropies. The commitment fuels CPI’s mission to accelerate the discovery and development of new medicines—such as vaccines and preventive drugs—to stop cancer before it starts.
This latest investment will help launch a $750,000 matching challenge, designed to expand philanthropic support for cancer prevention research and attract new champions to the field. Every dollar contributed will be matched, doubling the impact of each gift and propelling CPI’s next wave of discovery.
“Lyda Hill Philanthropies shares our belief that high-quality science can replace the fear around cancer with understanding and hope,” said Dr. Theodora Ross, President of the Cancer Prevention Initiative (CPI). “Their visionary investment in CPI’s mission brings us closer to a future where cancer prevention leads to longer, healthier lives for many.”
Founded on the belief that prevention is the most powerful form of cure, CPI funds innovative research aimed at intercepting cancer before it begins. The organization focuses on inherited cancers—where genetic predisposition provides a clear target for early intervention—and uses this lens to unlock insights that can lead to the prevention of all cancers.
“For me, this work is deeply personal,” said Howard Janzen, Chair of CPI’s Board of Trustees. “Like so many families, mine has been touched by cancer. Supporting CPI means investing in a future where our children and grandchildren won’t face the same risks. Lyda Hill Philanthropies’ continued partnership is helping make that future possible.”
Since its founding, CPI has invested nearly $5 million in hereditary cancer prevention research, providing critical early support when other funders may not take the risk. These catalytic investments enable scientists to generate the early data needed to pursue larger funding opportunities—creating pathways for transforming bold ideas into life-saving prevention tools.
The commitment from Lyda Hill Philanthropies builds on years of support and shared vision. Lyda Hill Philanthropies is known for its belief in “science benefiting humanity” and its focus on advancing breakthrough solutions that improve human health.
To learn more about the Cancer Prevention Initiative or to contribute to the matching challenge, email info@cancerpreventioninitiative.org, or visit www.cancerpreventioninitiative.org.
About the Cancer Prevention Initiative (CPI)
The Cancer Prevention Initiative (CPI) is a nonprofit organization dedicated to accelerating the discovery and development of new medicines that prevent cancer. CPI invests in early-stage, high-impact research that brings bold prevention ideas to life—supporting the scientists and innovations capable of stopping cancer before it starts. By focusing on inherited cancers as a model for all cancers, CPI partners with leading researchers and philanthropists to build a future where prevention is the norm, not the exception. To learn more, visit www.cancerpreventioninitiative.org.
About Lyda Hill Philanthropies
Lyda Hill Philanthropies encompasses the charitable giving for founder Lyda Hill and includes her foundation and personal philanthropy. The organization is committed to funding transformational advances in science and nature, empowering nonprofit organizations, and improving the Texas and Colorado communities. Because Miss Hill believes that “science is the answer” to many of life’s most challenging issues, she has chosen to donate the entirety of her estate to philanthropy and scientific research. For more details, visit lydahillphilanthropies.org.
Media Contact:
Contact: Marion Stewart–Thomas
Cancer Prevention Initiative (CPI)
Email: info@cancerpreventioninitiative.org
###
The Joy of Science: Interview with Nobel Laureate William G. Kaelin Jr., M.D.
CPI was fortunate to sit down for a conversation with Nobel Prize winner Dr. Bill Kaelin, from Harvard Medical School and the Howard Hughes Medical Institute (HHMI). We discussed topics ranging from training and motivation to discoveries, as well as the future of science and cancer prevention.
Biography
Dr. Kaelin received his BA and MD degrees from Duke University. He completed his residency in Internal Medicine at Johns Hopkins University School of Medicine where he was chief resident, and his clinical fellowship in Medical Oncology at the Dana-Farber Cancer Institute. His experience as a postdoctoral fellow in the laboratory of Dr. David Livingston at Dana-Farber was transformative in igniting and solidifying his interest in cancer research. He became an independent investigator at Dana-Farber in 1992. His work on the inherited cancer predisposition syndrome von Hippel–Lindau (VHL) disease established the VHL protein as critical for cellular oxygen sensing, and its dysregulation as a key step in the pathogenesis of kidney cancer.
Dr. Kaelin was elected to the National Academy of Sciences in 2010 and, together with Sir Peter Ratcliffe and Dr. Gregg Semenza, received the 2016 Albert Lasker Award for Basic Medical Research. The trio went on to share the 2019 Nobel Prize in Physiology or Medicine for their discoveries on how cells sense and adapt to oxygen availability.1
Dr. Kaelin is currently the Sidney Farber Professor of Medicine at the Dana-Farber Cancer Institute and Harvard Medical School and has been an HHMI investigator for over 25 years.
You have received arguably the most prestigious prize in science and medicine, but your start in laboratory science wasn’t great.
Right, my first research experience was in a physical chemistry lab as an undergraduate/pre-med student at Duke. At the end of the semester, the professor gave me a C-, which for a premed is like having a wooden stake driven through your heart. I was around 20 years old at the time, and it wasn’t as if this grade crushed a dream I had of becoming a scientist because I aspired to be a clinical doctor. But I decided this was a sign that I lacked the creativity and originality to work in a laboratory. Of course, 25 years later I can appreciate that it was not proof I lacked scientific talent, but at that time it certainly solidified my view that I should be a clinical doctor and not a scientist. As a result, I redoubled my efforts to become a clinician – which in hindsight I’m happy about, because I think too many people with an eye toward becoming physician-scientists go through their clinical training as sort of dabblers, convinced they won’t eventually become clinicians. I’m glad I approached my clinical training thinking I was going to be a clinician. It served me well later when I made the hard pivot to science.
What was the catalyst that made you think, “Maybe I can be a scientist”?
As a third-year medical student at Duke, I worked for a year studying tumor blood flow in the radiation biology lab of Randy Jirtle. Here, I published a couple of papers and I didn’t get a C-, which suggested to me that I might not be so bad at research after all. And I learned about both angiogenesis and the obscure disease von Hippel-Lindau disease, which would become very important to my career.
I’ve been to maybe three lectures in my life where I was almost levitating out of my chair because I knew I was having the privilege of seeing the future. One of them was in 1982, when Mike Bishop came to Duke and gave a talk about oncogenes—genes which when mutated or overexpressed contribute to the development of cancer—including several kinases. I remember thinking that as soon as we discover kinase inhibitors there is going to be a change in therapeutics forever. For the next 20 years people told me why this couldn’t be done – but thankfully, they were proven wrong, and kinase inhibitors are now key players in cancer treatment. Mike Bishop’s talk planted a seed.
When I was a resident at Johns Hopkins, one of my bicycle buddies, Eric Fearon, told me that I should grab lunch and listen to a young faculty member he was working with named Bert Vogelstein. That was another of these experiences. The prevailing wisdom at that time was that solid tumors were too heterogeneous and complex to study with molecular biology tools, so their use was largely limited to the study of blood cancers. However, Bert’s colon cancer studies were shattering that view and I was primed to believe that we were about to have a revolution in the application of molecular biology to cancer.
Also, one of my chairmen at Hopkins – Jack Stobo – did weekly bench to bedside talks and described molecular biology techniques like Southern blots and how to apply them in human genetics. In other words, there were several priming events that happened while I was in medical school and residency that kept me interested in cancer research.
When I came to Dana-Farber for my medical oncology fellowship I found my fellow fellows to be extremely accomplished from a scientific point of view. I think out of the eight people in my class, five or six were MD-PhDs. Several of them had published papers in the high-profile journals Cell, Science, and Nature. I remember Philip Kantoff was the star; he had published one of the early gene therapy papers. I was a lowly MD, voted “most likely to go into private practice”.
What were the early days of your independent career like?
As part of the fellowship training at Dana-Farber, there was an option to work in a lab for a couple of years. Although I didn’t think I was going to be a laboratory-based investigator, I thought I should at least work for a scientist who was good and famous. I tried desperately to get into Bob Weinberg’s lab, which had just cloned the RB tumor suppressor gene. He seemed interested but didn’t have space for a new person for another three years and I needed a spot in three months. While researching Bob Weinberg’s lab, I met a young guy named Shelly Bernstein who had trained with Bob Weinberg. Shelly was a pediatrician; he was very nice of course, all pediatricians are very nice, and he had just started his own lab which I joined. I had only been there for four months when he told me that he was shutting down his laboratory to go into clinical practice. Now I’m thinking that not only am I not destined to go into science but I’m causing other people to leave science!
My last clinical attending was David Livingston. While I was in Shelly’s lab, I picked up an article in Science magazine where a group had amplified part of the oncogene KRAS using PCR. PCR, or polymerase chain reaction, is a technique that can be used to make copies of specific regions of the genome. Just for fun, I tried doing the same following their protocol and it worked. I showed this to David. No one in David’s lab had ever done PCR so he immediately welcomed me into his lab and bought me a PCR machine. He told me that they’d just found that T antigen binds to the protein encoded by the RB gene that, when lost or altered, causes a childhood eye tumor called retinoblastoma. It seemed like everyone was working on RB. Bob Weinberg was working on RB, and now David’s working on RB. I think my expectations were so low it was easy for me to exceed them. In lab, I didn’t know enough to know the solutions to many problems, and I came up with my own solutions, some of which turned out to be better than the existing solutions. David was brilliant in every way a mentor could be brilliant. Both as a cheerleader and as a brilliant mind who had a great way of picking problems. One thing led to the next and I had some success in David’s lab.
When you started your own lab, you decided to focus on von Hippel-Lindau (VHL) disease. What spurred you into looking at VHL?
I was looking for something to work on that was different from what David was working on so I could establish my own scientific identity. I can still remember opening an issue of Science magazine and reading about the cloning of the VHL tumor suppressor gene (Latif et al., 1993)2. Sadly, one of the three corresponding authors of that paper just died this week – Michael Lerman from the National Cancer Institute (NCI). I thought this paper was it; this is what I want to work on for sure. I had worked on the RB tumor suppressor gene and thought I knew something about tumor suppressor genes. I also thought some of the approaches we had used for studying RB would be helpful in studying VHL.
At the time, there was a lot of excitement in molecular oncology for cancers like Burkitt’s lymphoma and Hairy Cell leukemia. These cancers were very interesting but relatively uncommon. I thought, if we were going to make a dent in cancer mortality, we needed to start tackling the common cancers. I knew that one of the cancers VHL gene mutation carriers develop is kidney cancer and kidney cancer is one of the ten most common cancers. I thought that working on VHL will allow us to learn about kidney cancer. I also knew from my stint in the Jirtle laboratory that VHL tumors are highly angiogenic and I thought studying VHL would teach us about the molecular control of angiogenesis, a topic of great interest in cancer therapeutics at the time because of Judah Folkman. I knew from my stint as a chief resident at Johns Hopkins that VHL tumors also cause excessive red blood cell production. What angiogenesis and increased red blood cell production have in common is that they are normally induced by low oxygen. This led me to assume that VHL must play some role in oxygen sensing and that these VHL tumors, in which the VHL gene is mutant, have hijacked the oxygen sensing pathway.
It turned out the assumptions about kidney cancer, angiogenesis, and oxygen sensing were all correct. From that point forward we didn’t have to do anything that was genius. We didn’t have to create any new technologies. We did our experiments competently and carefully. I think more than anything else, it was really seeing the connection between VHL and oxygen sensing that was the most important thing. And being lucky.
When you decided to pursue VHL, were you more motivated by the desire to help patients by working on a cancer that affected many patients, or by the intellectual challenge of solving a complex medical puzzle? Or both?
I didn’t think I was choosing between the two. I thought that VHL was a great puzzle—any time a gene or a protein was linked to cancer, that was interesting. I thought VHL was particularly compelling because of all the reasons stated above. I wanted to know why the loss of this gene so reproducibly caused cancers with almost 90% penetrance in these families and why these cancers produced high levels of the molecular distress signals normally induced by oxygen starvation. I figured why not work on a potentially important problem but also one that seemed like a good puzzle.
Your work on VHL has led to the development of drugs like belzutifan, which reverses the impact of a faulty VHL in cancer. At that time did you have thoughts that therapeutic development was a possible outcome?
My assumption at that time was that if we understood the VHL pathway, opportunities might arise for pharmacological intervention. We all knew of genetically validated cancer targets that were undruggable; for instance, it was not clear what to do with RB loss although we knew how it worked. Most drugs act by inhibiting their targets and very few bring mutated proteins back to life. From that point of view, VHL mutation, or worse, loss would normally be seen as “undruggable”. Nonetheless, it seemed possible that understanding the biochemical functions of the VHL protein would provide a path forward for pharmacologically mimicking its function or for exploiting vulnerabilities created when VHL function was lost. I hoped my research might lead to translational opportunities, but I knew it was not a given.
Except for your undergraduate research experience, you’ve had continuous research success– what do you attribute that to?
It is important to work on a good problem, pick a good project, find that question you’re so excited about that you can’t wait to go to work the next day. I always tell students that a nice fall back is to have genetics on your side, because at least you know you’re studying something that’s causal and not correlative. If you are doing clinical training, there are many clinical conundrums or medical paradoxes that are good places to start. Biological questions that map back to human diseases.
Usually, on the top on people’s list of questions I am now asked is “what’s the secret to winning the Nobel Prize?” Paradoxically, the secret to winning the Nobel Prize is not to think about winning the Nobel Prize. If you are picking good questions, doing your science well, having fun every day, and if you are very lucky, some recognitions like election to the National Academy or winning a Nobel might happen. But the real prize is the joy of doing science and the privilege of occasionally understanding things that have never been understood before, marveling at what nature is able to do. That’s the prize. And even better if your work actually helps patients. It’s not a bigger discovery or a better piece of science because someone put a blue ribbon on it – that’s a beauty contest.
If you set out to win one of these prizes or one of these other accolades, statistically, you’re going to become an embittered, unhappy person. Whereas, if you are doing your work for the right reasons and you’re very, very lucky you might win a prize now and then.
One of my favorites of the many questions I’ve been asked about the Nobel Prize is when I was in China. A reporter asked me, “Does winning the Nobel Prize make the imposter syndrome better or worse?” and my answer was “yes”. Of course, on one level you could say I got the brass ring, so I couldn’t have been so bad. But the minute one stops feeling a little imposter syndrome, it’s probably over in terms of future success. I think it’s important to have the right mixture of self-confidence and self-doubt.
If not the Nobel Prize, what gets you out of bed in the morning?
One of the many “David Livingstonisms” I like very much is that a good scientist should always think the most important thing they’re ever going to do lies ahead of them. I come to work every day with the idea that maybe one of the things we’re doing turns out to be important and useful. As a principal investigator, it is important for me to be fair to my postdocs who have entrusted their training to me. I have to believe any one of them could be doing the project that leads to that next really important thing. At any given time, I’m pretty pumped about the progress somebody is making in the lab. With our projects, I can easily imagine a trajectory that leads to something useful and impactful. I come to work with “I can’t wait to see what the next piece of data looks like.”
You are driven by this question you are passionate about, but how do you deal with downturns, times when it looks like nothing is working, and keep going?
I don’t take even the smallest successes for granted, like when the dye in the gel runs in the right direction. Celebrate even small achievements. It’s all magic.
I think one of the most important things for us mentors to do is to keep a close eye on the trainees who are doing all the right things, doing all the right experiments, but who are getting nowhere. Because it’s so important, especially for a young person, to have some taste of success within a reasonable timeline. I’ve seen that a little taste of success is enough to have people skyrocket. David was a big believer in putting talented young people into a fertile area and then watering them periodically. Sometimes, areas initially thought of as fertile turn out not to be and replanting will be necessary. As the mentor, I have the responsibility to find something else for them that will work. Sometimes it may look like things are going nowhere but you are very close, and you don’t know it yet. It can be really hard to know whether it’s a matter of persistence or whether it is just a dry well. You do get better with time at assigning probabilities of success in different projects. If a high-risk project has not yielded fruit within a reasonable length of time, it is sometimes important to switch to a “safer” project. It’s one of the things I think about a lot as a mentor; “how much failure can someone take?” But I’ve also been pleasantly surprised by how often “safe projects” have still led to really unexpected and exciting discoveries.
To be successful you need to pick a good project – a question that excites you and one that is meaningful— be positive, be persistent, and especially if you are a young researcher, choose the right mentor. Anything else?
You know how most jokes have an element of truth to them? There’s the old joke that one of the best predictors of winning a Nobel Prize is having trained with someone who has won the Nobel Prize. Turns out, it’s literally true, mostly for physics and chemistry but also somewhat for medicine. There is something in the training or the way of thinking that’s hard to capture in writing – I call it scientific intuition. David had a great nose for a good problem. On the flip side he also had a great nose for bullshit. He could go to a lecture and within 5 minutes turn to me and say that it’s complete bullshit. I have to be careful because this is all subjective, but I certainly meet scientists around the world who I’m sure are smarter than me and more technically capable than me, but they don’t have my scientific instincts and taste. And I find myself asking “why are you doing this, why are you working with this?”
The issue of pedigrees is interesting because by valuing pedigrees we can miss talented people who didn’t have opportunities for impressive pedigrees.
That is a great comment. I think to succeed you have to have the right balance of self-confidence and self-doubt as I have already said. They’re equally important, and it is not great to miss one or the other. I think if you’ve trained at a great place or if you’ve trained with a great person, you’re more willing to ask audacious questions. Because you think “who else is going to do it? of course, I’m going to do it.” Especially when I’m visiting people at places outside of Harvard, I provide encouragement that they are more capable than they think. They don’t have to go to Harvard to be talented and often just need a dose of confidence. It’s really getting the balance of confidence and self-doubt right. It’s sort of like the end of Wizard of Oz when they hand you the certificate that says you did this. Part of it is just having that extra gear that makes you a little bit more audacious. That’s why I say, to do significant work, it helps to be in a place that believes in you and supports you.
We want to ask you about the trend toward “team science.” Collaboration is important but on the other hand it can encourage group thinking and herd mentality. How do we maintain scientific integrity and original ideas in the midst of needing to have team science?
I’m always careful when answering a question about what to work on and whether to do it as part of a team not to be overly prescriptive, like you should do this type of science or that type of science. What is important is that you do the type of science that excites you; what is satisfying to one person may not be satisfying to another.
I have learned from sociologists that at one extreme are scientists they call the “lone hunter gatherer scientists.” They tend to dominate in the early stages of science – many lone hunter gatherer scientists going in different directions, following their noses, and the hope is that a couple of them will come back with something useful. As science matures and becomes more resource intensive and sometimes a little like engineering, the “communal harvesters” start to come in, and they start to displace some of the lone hunter gatherer scientists. They both have strengths and weaknesses. I am a lone hunter gatherer scientist— I want to work on my problem the way I want to work on it.
One of quotes in “Time, Love, and Memory”4 – a biography of Seymour Benzer– is that a good experiment should be pretty and witty. I see a lot of team science that is done because they have mega resources, such as access to precious samples and powerful technologies. When these things are put together, they can generate something publishable. I’m not saying it isn’t useful, but that’s a different kind of science than trying to see if you can solve a puzzle by tinkering in the laboratory and thinking about it deeply and in different ways. I like the science where I think “why, that person was really clever, I wish I had thought of that” as opposed to “if I had that machine and those samples, I could have done that”.
A lot of drug discovery, at least in the past, came from hunter gatherer-type science. It’ll be interesting to see with this new big science if we can come up with new drugs.
I think it is important to view cancer research activities as being scientific, engineering or both. I think it is especially important for funders and policy makers to identify that. Rick Klausner opened my eyes to this, that the reason President John Kennedy could say “we’re going to put a man on the moon in 10 years” is because it was fundamentally an engineering problem. When it’s an engineering problem, the timelines and the deliverables are predictable, and one can estimate the time and cost, as opposed to science where the timelines and deliverables are usually unpredictable.
Industry is really good at taking on certain engineering aspects – taking a paradigm that you know works and scaling it with resources, as opposed to the real out-of-the-box early science that I think we should be doing in academia. That’s why I’m a little sad that so many academic scientists are being coerced into doing things that feel better suited for industry.
The VHL story is great because it reflects what CPI aims to do – support basic biology in the hope that it will help develop medical interventions to prevent disease in the future. It sounds like you endorse CPI’s strategy.
Yes, I am a strong advocate for basic and fundamental work. Discoveries and opportunities come from unexpected places. When people come to me and say aunt Sadie died of cancer X so I want to give money to someone who works on cancer X, I say you can do that but if I’m a betting person I would bet that the next big breakthrough for cancer X will come from someone who is working on cancer Y or frankly from someone who doesn’t even know they are working on cancer. That someone could finally give us the last puzzle piece of basic knowledge that was missing. Now we can go back to cancer X and do something significant. You also have to be a little opportunistic and look for opportunities for prevention.
On the topic of prevention, do you think that belzutifan could be used to prevent cancers, particularly in VHL patients?
The challenge for prevention drugs is safety. The level of toxicity acceptable when treating a cancer patient is very different from what is acceptable in a prevention setting, where the drug is given to healthy individuals. In this regard, VHL patients were reluctant to be treated in a preventative setting with VEGF tyrosine kinase inhibitors because of their toxicity. Belzutifan seems better tolerated in this population.
Actually, belzutifan is already being used preventatively in the VHL population although it’s not marketed as such. A study published this year3 (Srinivasan et al., 2025; Figure 1) shows the effectiveness of belzutifan for prevention in the VHL population. A truism in medical oncology is that most drugs work better in frontline setting. In this trial, they had 61 VHL patients with measurable kidney tumors, who were never treated with drugs or radiation. They were under surveillance for four years at the NCI before they were put on belzutifan. During these four years prior to belzutifan, the patients had to go to the operating room often to have tumors removed. But once they were put on belzutifan the surgeries effectively stopped. It’s not completely zero, but it’s pretty close. It is a very impressive result. (Please see Figure 1 in the attached pdf).
What have you been involved in recently that you are particularly proud of?
Something I have been excited about recently are the GLP-1 drugs. I have been a member of the Eli Lilly and Company board since 2012. And I am proud to say that I was one of the people in 2015-2016 who convinced the board and management that there was more to obesity than simple lifestyle choice. I think we’re going to see a significant decrease in obesity in the next 10 to 20 years. Thank goodness for people like Joel Habener and others who had done the basic science around GLP1. This is another example of how basic science contributes to the development of new targeted interventions and how discoveries come from unexpected areas of research.
Thank you for an amazing conversation!
Disclaimer: Dr. Kaelin has a financial interest in belzutifan. He is not directly involved in the clinical trials of the drug.
References
- https://www.nobelprize.org/prizes/medicine/2019/summary/
- Latif et al., 1993. Science. Identification of the von Hippel-Lindau disease tumor suppressor gene.
- Srinivasan et al., 2025. Lancet Oncology. Belzutifan for von Hippel-Lindau disease-associated renal cell carcinoma and other neoplasms (LITESPARK-004): 50 months follow-up from a single-arm, phase 2 study.
- Time, Love, and Memory: A Great Biologist and His Quest for the Origins of Behavior is a biography of the great Seymour Benzer, Ph.D., a pioneer in molecular and behavioral genetics, by the Pulitzer Prize-winning author Janathan Weiner.
Von Hippel Lindau (VHL) disease is a hereditary disease that increases the risk in carriers of various cancers, including clear cell Renal Cell Carcinoma (ccRCCs). It is caused by inherited mutations in the eponymous tumor suppressor gene VHL. It is considered a rare disease affecting around 1:35,000 people globally. Since patients develop multiple tumors from a young age, and most show symptoms by age 30, they are typically enrolled in surveillance programs with MRI scans every 3–4 months to detect new tumors or changes in existing ones. Often, as a preventive measure, tumors are removed by surgery.
The name “VHL” was coined in 1936, based on the descriptions of the disease by Eugen von Hippel and Arvid Lindau. The VHL gene itself was identified in 1993. Until then, VHL disease was considered a rare curiosity with little clinical relevance and no clear connection to wider studies of cancer.
Belzutifan is a drug that blocks the protein HIF-2alpha. Under normal circumstances, HIF-2alpha helps cells adapt to low oxygen levels. However, in certain cancers HIF-2alpha builds up to abnormal levels due to VHL mutations. By blocking HIF-2alpha function, Belzutifan blocks tumor growth.
Theo Ross: 2024 Women in Biopharma R&D
Theo Ross, M.D., Ph.D. CPI’s, President and Chief Scientific Officer, was recognized as one of 20 women making an impact in Biopharma Research & Development in 2024 by Endpoints News. Dr. Ross serves as Vice President of Early Oncology R&D at AbbVie. Read about her journey from medical school to pharma and how empathy drives her work.
Conference BRCA 30 Years: Discovery to Impact
Nov 4-5, 2024 – Hybrid Event
The Women’s College Hospital (WCH) has organized a special hybrid conference to celebrate the 30-year anniversary of the discovery of BRCA genes. The conference will cover research and innovations related to BRCA genes and BRCA-related inherited cancers. Many prominent cancer researchers and oncologists, including CPI scientist Dr. Joanne Kotsopoulos, will present their work at this event.
We encourage you to attend this event in person or virtually to learn how the discovery of BRCA genes has influenced cancer research and cancer patients. DAY 1 caters mainly to researchers and healthcare providers and DAY 2 to patients and their families. Please see the links and documents below for more information.

Damon Runyon Fellowship Award
CPI has partnered with Damon Runyon Research Foundation to promote research relevant to the development of molecular approaches (such as drugs and vaccines) for the prevention of inherited cancers. If an applicable proposal is selected by Damon Runyon’s award selection committee and approved by the Damon Runyon Board of Directors, CPI will co-fund the Fellowship Award.
Award Overview – https://www.damonrunyon.org/for-scientists/application-guidelines/fellowship
Application Guidelines – https://www.damonrunyon.org/for-scientists/application-guidelines/fellowship/forms
Projects considered for funding by CPI are those that have the potential to make significant contributions to the development of chemo- or immuno-prevention measures that could reduce the risk of cancer in germline mutation carriers. Discovery research that could increase the understanding of early, pre-cancer stages are also considered. Visit the link below for more information on CPI’s funding priorities.
https://www.cancerpreventioninitiative.org/apply-for-grants/funding-priorities/
We encourage postdoctoral researchers with novel and innovative ideas related to precision prevention of inherited cancer to take advantage of this opportunity. Please contact Grants@CancerPreventionInitiative.org with questions regarding the CPI-funded award.
In Memory of Dr. Charis Eng
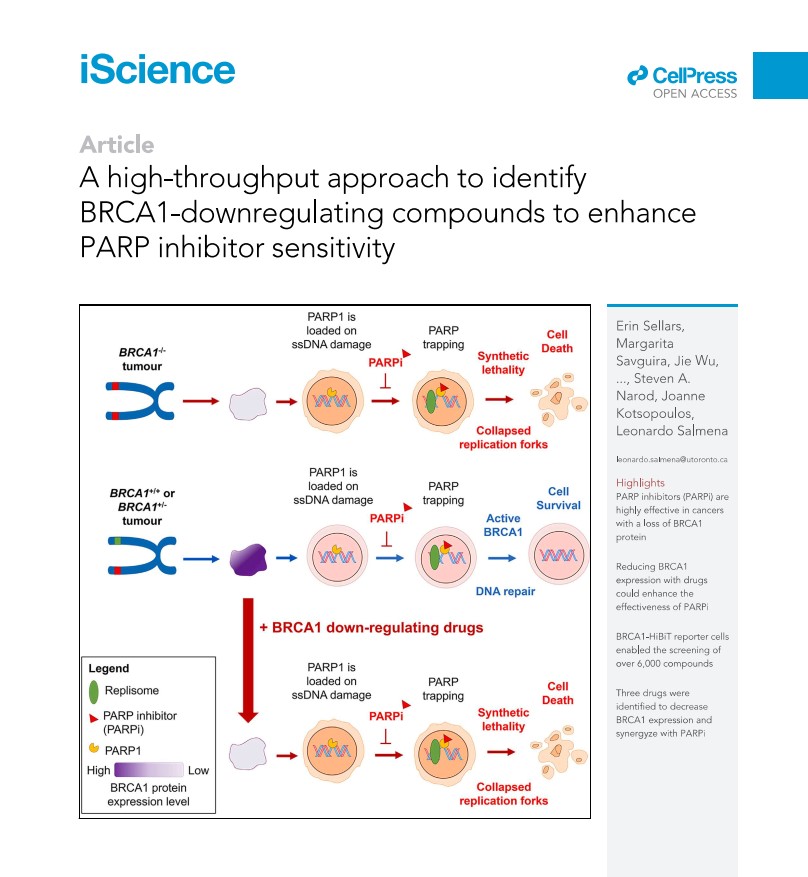
A high-throughput approach to identify BRCA1-downregulating compounds to enhance PARP inhibitor sensitivity
A CPI grant funded Dr. Kotsopoulos at the University of Toronto, Toronto, Canada for Evaluating BRCA1 haploinsufficiency as a putative target for the prevention of BRCA1-associated cancer. She and her collaborators developed a cell-based test to screen for drugs, small molecules, or natural compounds that could alter BRCA1 levels. Following the screening of more than 6,000 compounds using this assay, they identified several agents that can decrease BRCA1 protein levels. Some of these compounds can sensitize breast cancer cells to the PARP inhibitor Olaparib and may therefore have future clinical utility.
Read the full article in iScience.
Li Fraumeni Syndrome and one family’s harrowing experience with this deadly disease
Li Fraumeni (LF) is a hereditary cancer syndrome due to deleterious inherited mutations in the TP53 gene that increases the risk for developing a wide range of cancers, mostly sarcomas, breast cancers, brain tumors, and leukemias.
In the Wall Street Journal article below, journalist Lawrence Ingrassia writes about the multiple deaths in his family from a then unknown cause, and the scientists whose dedicated research spanning decades that eventually unearthed the culprit.
Much has been learned about LF since the death of the author’s mother in the 1950’s; when the author’s brother died after developing multiple cancers in 2019, he knew that he carried a TP53 mutation. However, the disease is still managed in mutation carriers by frequent screenings and tests to catch the cancers as early as possible. There is currently no way to prevent the disease before cancer(s) have taken hold.
As such, CPI funded a project by Dr. Jos Jonkers that could lead to vaccines that prevent cancers with TP53 mutations.
Solving the Cancer Mystery That Devastated My Family
For decades, Lawrence Ingrassia wondered why so many of his loved ones got cancer. Then a team of dedicated researchers discovered the gene p53.
By Lawrence Ingrassia
My most enduring childhood memories of my mom are of her being sick. Of visiting her in the hospital with my older brother and two younger sisters. Of our grandmother staying with us while our mom recuperated from breast cancer surgery. Of seeing her in bed at home with a soulful, sad look on her face.
She had been ill, sometimes gravely, off and on while I was growing up. I’m pretty sure that she first had cancer as early as 1958, when she was 32, though my memory is vague because I was only 6.
2023 CPI Research Meeting
The second Cancer Prevention Initiative (CPI) Research Meeting was held on January 18th, 2023. Following the success of the first meeting in 2021, this event was again held virtually and was moderated by Dr. Larry Brody, Director of the Division of Genomics at the National Human Genome Research Institute at the National Institutes of Health. He is a strong advocate for cancer prevention and has made pioneering discoveries of the genetic basis of breast cancer and the roles of the breast cancer genes BRCA1 and BRCA2.
CPI President and Chief Scientific Officer Dr. Theo Ross opened the meeting by welcoming the attendees and thanking Dr. Brody for moderating the event again this year. She reiterated the mission and the strategy of CPI, to accelerate the discovery and development of new medicines that prevent cancer by supporting research on the prevention of inherited cancers. She shared the good news that in addition to the progresses made in the scientific research front, CPI has successfully raised substantial funds to continue support of current projects as well to as start additional projects this year. She also spoke of new funding opportunities in the external cancer prevention front: concept proposals by the National Cancer Institute’s Division for Cancer Prevention in support of research related to immunoprevention and the discovery of natural compounds that may prevent cancer. This is a welcome change, as prevention research has historically received weak support from funding agencies. Even today, only a small fraction of the funding is devoted to prevention, and treatment remains the main focus. These new efforts, though small, may herald a rising interest in prevention by funding agencies.
The 2023 CPI research meeting featured a lineup of CPI-funded researchers who presented updates on their research projects. The first session of the meeting was dedicated to research projects on immunoprevention of cancer, harnessing the abilities of the immune system to stop precancerous lesions from developing into cancer. Dr. Peter Lee of the City of Hope Comprehensive Cancer Center discussed his project related to repurposing an FDA-approved antiparasitic drug that they showed could kill nascent tumor cells in a way that activates the immune surveillance system to prevent future cancer initiation.
The next presenter, Cleveland Clinic’s Dr. Charis Eng, started her presentation with a historical imperative for prevention from the ancient Chinese medical text Huang Dee Nai-Chang: “Superior doctors prevent the disease, mediocre doctors treat the disease before evident, and inferior doctors treat the full-blown disease”. This philosophy resonates with the mission and vision of CPI to shift the approach to cancer from treatment to prevention. Dr. Eng and her team are working on developing a vaccine that would specifically target BRCA1 mutated cells before they can proliferate into harmful tumors and can be given to BRCA1 mutation carriers to reduce their chance of developing cancer. Along the way, they have generated the first gene expression data comparing tumor and normal mammary tissue of BRCA1 mutation carriers. These data are an invaluable resource for all researchers studying breast cancer.
The second session was dedicated to projects exploring the earliest events that drive cancer initiation and understanding the mechanisms underlying these events. BRCA1 mutation carriers have only one “good” copy of BRCA1 instead of the normal two. It is well known that precancerous cells develop when the “good” copy of the BRCA1 gene is lost. Dr. Maria Jasin and her team at Memorial Sloan Kettering Cancer Center have generated a very elegant cell-based assay to identify compounds and signaling pathways that contribute to BRCA1 gene loss. Their work can lead to finding ways to intercept this early step necessary for transformation.
CPI-funded researchers at the Women’s College Research Center at University of Toronto, Drs. Joanne Kotsopoulos and Leonardo Salmena, and Ph.D. candidate Erin Sellars, attempt to prevent cancer development in BRCA1 mutation carriers by restoring BRCA1 expression levels to normal levels. They used a high-throughput screen they developed to identify drugs that increased BRCA1 expression, and they have hit upon some promising targets.
The CPI Research Meeting was an opportunity for CPI scientists to share their newest data and get productive feedback from fellow scientists. It was also an opportunity for cancer scientists with a shared interest in prevention to come together and have a larger conversation on the challenges of carrying out cancer prevention research – from limited funding and lack of enthusiasm from the medical community to restrictions posed by regulatory agencies. These are some of the challenges CPI attempts to address through its goals.
The meeting ended with closing remarks by Dr. Ross.
The meeting was supported by generous funding from Lyda Hill Philanthropies.
Moderator:
Lawrence Brody, Ph.D.
Director, Division of Genomics
National Human Genome Research Institute
National Institutes of Health
Participants:
Charis Eng, M.D., Ph.D. Presenter
Professor, Sondra J. and Stephen R. Hardis Endowed Chair in Cancer Genomic Medicine
Lerner Research Institute, Cleveland Clinic
“Transcriptome guided vaccine for BRCA1/2 germline mutation carriers”
Maria Jasin, Ph.D. Presenter
Professor, Lab Head
Memorial Sloan Kettering Cancer Center
“Preventing LOH in BRCA mutation carriers”
Joanne Kotsopoulos, Ph.D.
Scientist, Familial Breast Cancer Research Unit, Women’s College Research Institute
Associate Professor, Department of Pharmacology & Toxicology, University of Toronto
“Screening for modifiers of BRCA1 expression”
Peter P. Lee, M.D. Presenter
Chair, Department of Immuno-Oncology
Professor, Department of Hematology & Hematopoietic Cell Transplantation
City of Hope Comprehensive Cancer Center
“Chemo-immunoprevention for cancer via repurposing a low-cost, safe, anti-parasitic drug”
Steven Narod M.D., FRCPC, FRSC
Tier 1 Canada Research Chair in Breast Cancer, Women’s College Research Institute
Professor, Dalla Lana School of Public Health, University of Toronto
Ying Ni, Ph.D.
Assistant Professor, Cleveland Clinic Center for Immunotherapy and Precision Immuno-oncology
“Transcriptome guided vaccine for BRCA1/2 germline mutation carriers”
Leonardo Salmena, Ph.D.
Associate Professor, Department of Pharmacology and Toxicology, University of Toronto
Affiliate Scientist, Princess Margaret Cancer Centre
Canada Research Chair, Tier 2
“Screening for modifiers of BRCA1 expression”
Erin Sellars, M.Sc. Presenter
Ph.D. Candidate, Salmena Lab
Department of Pharmacology & Toxicology, University of Toronto
“Screening for modifiers of BRCA1 expression”
CPI team participants:
Doug Hager, Ph.D.
CPI Sr. Vice President, Project Management and Operations
Theo Ross, MD, Ph.D.
CPI President and Chief Scientific Officer
Marion Stewart-Thomas, M.S.
CPI Operations Manager
Angelique Whitehurst, PhD.
CPI Sr. Scientist and Advisor
Ranjula Wijayatunge, Ph.D.
CPI Project Manager